AI Workflow Automation for Healthcare Operations (2026)
AI workflow automation for healthcare operations applies machine learning and rules-based routing to handle high-volume administrative and clinical tasks - patient intake triage, prior authorization, and compliance reporting - without manual intervention at every step. US clinics and health plans deploying these systems in 2025-2026 report measurable reductions in administrative overhead, but the technology introduces HIPAA risk vectors that require a deliberate AI data governance framework before go-live. The same automation pattern - structured data in, model classification, automated action or human review queue, full audit log - is now being adopted by mid-market finance and FP&A teams for report generation, reconciliation, and data-pipeline orchestration, with SOX, GDPR, and PIPEDA replacing HIPAA as the governing compliance layer.
Key Takeaways
Patient intake AI routing reduces time-to-triage at mid-market US clinics, but only when training data reflects the actual patient population without demographic bias
Prior authorization automation cuts staff burden when AI pre-screens submissions rather than replacing clinical review entirely
HIPAA (US), GDPR (UK/EU), and PIPEDA (Canada) impose distinct requirements on AI vendors - data residency, consent mechanisms, and audit trails differ by jurisdiction
Microsoft Fabric Lakehouse for healthcare analytics is the emerging data layer standard for multi-payer AI deployments that need a unified, auditable data store
The most consistent AI workflow failure points are model drift after 90-180 days, edge case misrouting, and EHR integration instability - all preventable with deliberate architecture
AI workflow automation for finance teams introduces an additional compliance layer: SOX Section 302/906 requires every automated financial control to be documented, tested, and auditable as an IT general control before it touches the close cycle
What Is AI Workflow Automation for Healthcare Operations?
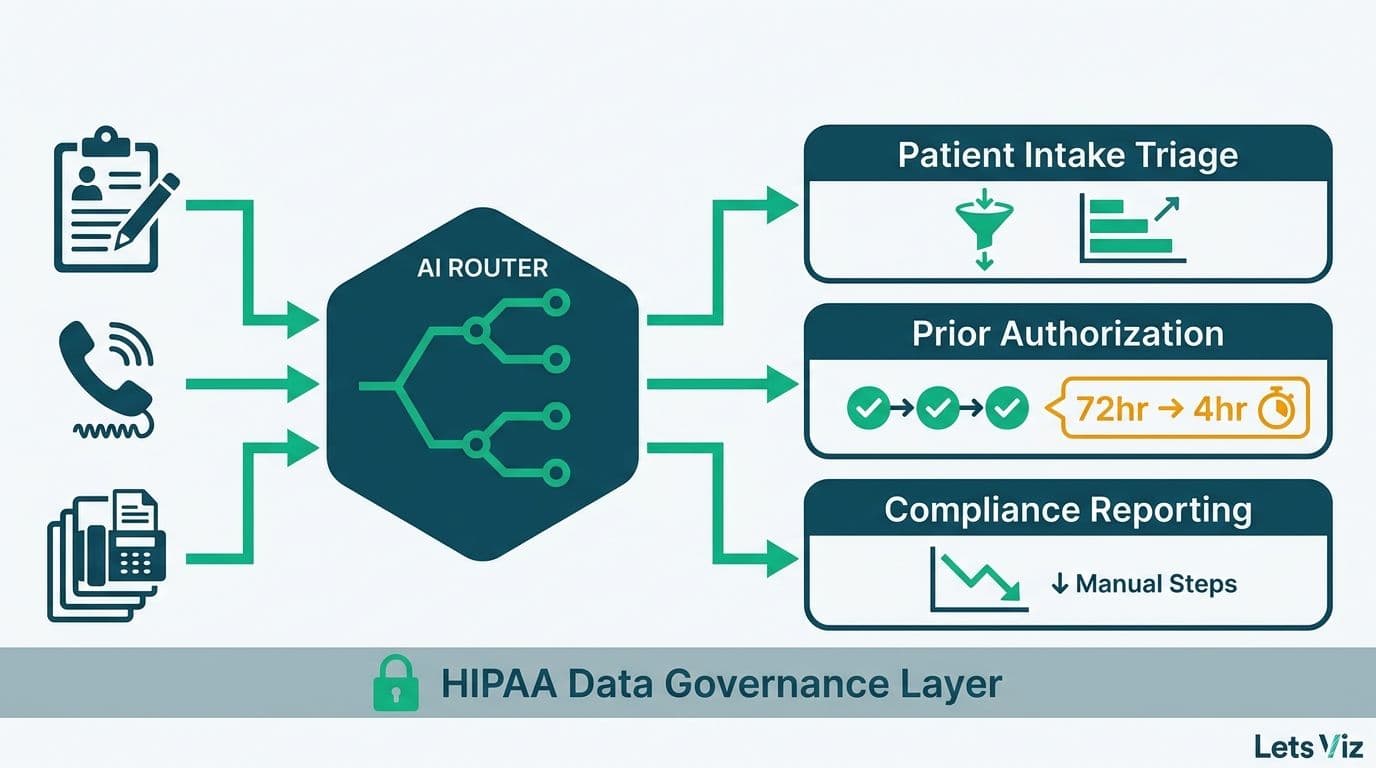
AI workflow automation for healthcare operations refers to systems that apply machine learning models, NLP pipelines, and rules engines to route, process, and report on clinical and administrative events without manual handling of every case. The underlying pattern is consistent across use cases: structured data enters the system, a model assigns a classification, the result routes to an automated action or a human reviewer queue, and every decision is logged for audit.
The scale of investment reflects how seriously health systems are treating this shift. The Healthcare Financial Analytics Market is projected to grow at an 8.58% compound annual growth rate from 2025 to 2035, according to Market Research Future (2025), driven by regulatory pressure, value-based care contracting, and the operational burden of fragmented EHR and payer data.
For CIOs and data leads evaluating where to start, AI automation consulting typically begins with a workflow audit - mapping tasks by volume, repetitiveness, and decision-rule clarity. The three workflows that consistently return the fastest payback at mid-market health systems are patient intake routing, prior authorization processing, and compliance reporting. Each has different data requirements, distinct regulatory exposure, and specific failure modes that need to be understood before implementation begins.
How Are US Clinics Deploying AI for Patient Intake Routing?
Patient intake routing is the process of assigning an incoming patient to the right care pathway, urgency level, and provider type. At most mid-market US clinics, this is a manual triage step performed by front-desk staff or nurses. AI automates the initial classification layer, allowing human reviewers to focus on edge cases and complex presentations rather than every submission.
The deployment pattern at a US regional health system running five to fifteen outpatient locations typically works as follows: a patient submits a reason-for-visit through the patient portal, an NLP model classifies the free-text complaint against historical ICD-10 coding patterns, and the system routes the case to a care team type, urgency queue, and appointment slot before any human reviews it. Confidence-weighted outputs below a defined threshold - typically 80% - route to human review rather than automatic placement.
MedInsight's 2025 healthcare analytics roundup identified AI-driven analytics and value-based care as two of the three defining themes reshaping health system operations across the US, with payer analytics innovation completing the top three. Intake routing sits at the intersection of all three: it directly affects utilization patterns and feeds the performance data that value-based care contracts rely on for attribution and quality scoring.
The critical failure mode: training intake AI on historical triage data without auditing for demographic bias. Historical intake decisions often reflect documented disparities in clinical practice across patient demographics. A model trained on biased historical data replicates that bias at the scale of every future routing decision. Demographic disparity audits are a regulatory expectation under CMS guidance for AI-assisted clinical decisions in Medicare Advantage plans - not an optional enhancement.
For Canadian health systems, implementation adds a consent management layer. Under PIPEDA and provincial legislation such as Ontario's Personal Health Information Protection Act (PHIPA), patient consent to AI-assisted routing must be explicit and revocable. A mid-market Ontario clinic group deploying intake AI in 2025 found that designing and testing the consent architecture added six weeks to the implementation timeline - time that must be planned into the project schedule from the outset, not discovered mid-deployment.
How Does AI Workflow Automation Handle Prior Authorization?
Prior authorization is the process by which a provider must obtain health plan approval before delivering a service or prescribing a medication. It is among the most document-intensive administrative workflows in US healthcare, consuming substantial clinical staff time on documentation, phone outreach, and appeals processing.
AI workflow automation for prior auth follows this standard pattern:
The EHR or practice management system flags a service requiring authorization based on the CPT or HCPCS code
An AI classification model checks current payer coverage rules - via real-time API or a synchronized payer rule database - and categorizes the request as likely-approved, likely-denied, or peer-review-required
Likely-approved requests auto-submit with supporting clinical documentation extracted from the EHR record
Peer-review and likely-denied cases are queued for a human reviewer, pre-populated with recommended supporting evidence and payer-specific appeal language
This is not a replacement for clinical judgment. It is a pre-screening layer that reduces the volume of cases requiring direct staff handling from 100% to roughly 20-30%, freeing clinical staff for higher-complexity cases and direct patient interaction.
The failure mode that catches most teams off guard: payer rule drift. Health plans update coverage criteria - sometimes quarterly. An AI model trained on last year's payer rules will generate incorrect classifications for updated policies. This is a rule-base synchronization problem, not a model retraining problem, and the two require different engineering approaches. Teams that conflate them discover the distinction when authorization accuracy degrades months after the initial deployment, often after thousands of incorrect classifications have already been generated.
A UK National Health Service trust piloting AI-assisted prior auth for specialist referrals in 2025 encountered a related challenge: the model performed accurately against baseline pathways but degraded when specialty-specific criteria changed mid-year. Under GDPR Article 22, the trust was also required to ensure patients could request human review of any automated decision affecting their clinical pathway - an explainability requirement that had to be built into the system architecture from the start, not retrofitted after launch.
What HIPAA Guardrails Apply to AI Workflow Automation in Healthcare?
HIPAA compliance defines the baseline architecture for any AI system that processes protected health information (PHI) in a US healthcare context. The guardrails that matter most for AI workflow automation are specific, non-negotiable, and frequently underestimated in initial scoping.
Business Associate Agreements (BAAs). Every vendor in the AI pipeline that handles PHI - including the model provider, cloud infrastructure, and any orchestration middleware - must sign a BAA. This includes large language model providers used for NLP tasks within the workflow. As of 2026, not all major LLM providers offer HIPAA-eligible service tiers with BAAs. Verify vendor status at the contract stage, not after the implementation is underway.
Minimum necessary standard. AI models must be designed to use only the PHI required for the specific task. A prior authorization model does not need a patient's complete social history. A triage routing model does not need billing records. Data access scope must be defined at the pipeline design stage - retroactive restriction is technically and operationally expensive.
Audit trails. Every automated decision that touches PHI must be logged with a timestamp, the data inputs used, the model version that generated the output, and the routing result. This is the minimum required for CMS audits and breach investigations. Our AI analytics data privacy guide for healthcare covers audit trail architecture in detail, including the log schema recommended for HIPAA compliance reviews.
De-identification for training data. HIPAA's Safe Harbor standard - removing 18 specified identifiers - or the Expert Determination method applies to any PHI used in model training. Many health systems supplement with synthetic data generation to build statistically representative training sets that carry no PHI risk. The HIPAA-compliant analytics dashboard best practices checklist covers how these requirements interact with the analytics and reporting layer.
Canadian organizations operate under PIPEDA federally, with provincial health information legislation adding requirements in Ontario (PHIPA), Alberta (HIA), and British Columbia (PIPA). The material difference from HIPAA: PIPEDA mandates documented data flow maps and a Privacy Impact Assessment (PIA) before deploying any system that processes personal health information. Build the PIA into the project timeline from day one - it is a prerequisite for deployment, not a post-launch documentation exercise.
How Does AI Workflow Automation for Finance Teams Accelerate FP&A and Compliance Reporting?
The same architectural pattern driving healthcare operational efficiency - structured data in, rules-based or ML classification, automated action or human review queue, immutable audit log - maps directly onto the highest-volume pain points for mid-market finance and FP&A teams: monthly close cycles, variance reporting, multi-system reconciliation, and SOX-controlled financial disclosures.
Report generation. FP&A teams at companies running 200-2,000 employees typically spend 30-50% of analyst time assembling management reports from ERP exports, CRM pipeline data, and data warehouse aggregates before any analysis begins. AI workflow automation for finance teams eliminates that mechanical assembly layer: a pipeline monitors upstream data sources, detects when period-end snapshots are available and pass defined quality thresholds, triggers a generation step that pulls pre-mapped fields into a report template, flags material variances against prior period and budget, and delivers a first-draft pack to the finance lead for review and sign-off. The analyst role shifts from data janitor to variance interpreter - a much higher-value use of the function.
Reconciliation. Matching transactions across the general ledger, bank feeds, accounts payable sub-ledger, and third-party payment processors is repetitive and rule-based - exactly the conditions where AI automation outperforms manual processing. An AI reconciliation layer classifies each unmatched item by likely cause (timing difference, duplicate, coding error, genuine discrepancy), auto-resolves high-confidence matches, and queues exception items for human review with supporting context already populated. Teams that deploy this pattern typically reduce reconciliation cycle time by 60-70% and find that the human review queue contains only the genuinely ambiguous items rather than the full transaction population.
Data-pipeline triggers. Finance workflows frequently stall because downstream steps run on fixed schedules rather than on data readiness signals. AI-driven pipeline orchestration monitors upstream data quality metrics - completeness, referential integrity, outlier thresholds - and triggers downstream steps only when the data meets defined criteria. This eliminates the manual handoff emails and status-check meetings that currently coordinate close cycle dependencies at most mid-market finance teams.
SOX compliance architecture. For US public companies and their subsidiaries, Section 302 and Section 906 certification requirements mean that any AI automation touching financial close processes must be scoped and documented as an IT general control (ITGC). Practically, this means: model changes require change management documentation and testing evidence before promotion to production; automated reconciliation steps must map to a documented control objective with defined exception-handling procedures; and the audit trail must be sufficient for external auditors to trace any reported figure back to its source data and the automated logic that processed it. SOX compliance is not a post-deployment retrofit - it must be designed into the control architecture from the initial scoping phase, in the same way HIPAA minimum necessary requirements must be designed into healthcare AI pipelines before the first data flow is mapped.
GDPR and PIPEDA data handling. Finance data in EU and UK operations frequently contains personal data - employee payroll records, customer payment information, vendor contact details embedded in invoice metadata. GDPR Article 5 data minimization principles apply to any AI model trained on or processing this data: the model must use only the personal data necessary for the reconciliation or reporting task, and data subjects retain rights of access and erasure that must be technically implementable. Canadian finance teams operating under PIPEDA face the same documented data flow map and PIA requirements that apply to healthcare AI deployments - the regulatory instrument is the same; only the data category changes.
For finance teams evaluating where automation returns the fastest payback, the starting point is the same as healthcare: a workflow audit that maps tasks by volume, repetitiveness, and decision-rule clarity. Reconciliation and variance flagging consistently return the fastest measurable payback. SOX-controlled report generation returns the most significant risk reduction - replacing manual assembly steps with auditable, version-controlled automation removes a material class of human error from the close cycle.
Which Analytics Infrastructure Supports AI Workflow Automation in Healthcare?
AI workflow automation generates structured output - routing decisions, confidence scores, model version identifiers, audit logs, and performance metrics - that requires a queryable, auditable data layer. The analytics infrastructure decision shapes how governable the AI system is from day one, and how easily leadership can monitor performance, detect drift, and demonstrate compliance during regulatory reviews.
Microsoft Fabric Lakehouse for healthcare analytics is the architecture pattern gaining the most traction at mid-market US and Canadian health systems in 2025-2026. A Fabric Lakehouse consolidates structured claims data, semi-structured EHR exports, and unstructured clinical notes in a single OneLake storage layer, then serves BI dashboards, ML training pipelines, and compliance reports from that unified source of truth. The medallion architecture in Microsoft Fabric - bronze for raw ingestion, silver for de-identified and validated data, gold for analytics-ready aggregates - maps directly onto HIPAA minimum necessary and audit trail requirements, making it particularly well-suited to multi-payer healthcare AI deployments. The same medallion pattern applies cleanly to finance AI deployments, where the silver layer enforces SOX-relevant data quality controls and the gold layer feeds auditor-ready reporting aggregates.
For teams simultaneously evaluating BI platform options - weighing Looker vs Power BI vs Tableau for dashboard delivery, or assessing when to migrate from Tableau to Power BI as part of a broader Microsoft Fabric build - the data layer decision comes first. A well-structured Lakehouse serves any BI consumer from the gold layer, which means the visualization platform choice does not constrain the analytics architecture.
AI data governance framework requirements for healthcare AI deployments:
| Governance Layer | What It Covers | Healthcare-Specific Requirement |
|---|---|---|
| Data access controls | Who can query PHI under what conditions | Role-based access tied to clinical workforce function |
| Model registry | Version tracking for all deployed models | Audit trail for CMS reviews and HIPAA breach investigations |
| Lineage tracking | Data origin and transformation history | HIPAA minimum necessary compliance documentation |
| Explainability | Why the model made a specific routing decision | GDPR Article 22 (EU), CMS AI guidance (US) |
| Drift monitoring | Model performance over time | Revalidation triggered every 90 days at minimum |
The AI consulting services market is projected to grow from $11.07 billion in 2025 to $90.99 billion by 2035 at a 26.2% CAGR, according to Future Market Insights (2025). A significant portion of that growth reflects health systems and finance organizations engaging external expertise to build exactly these governance frameworks - the technical infrastructure exists, but the governance architecture requires domain knowledge that most internal data teams are still developing.
Where Does AI Workflow Automation for Healthcare Still Fall Short?
Realistic implementation planning requires confronting where these systems fail. The failure modes are consistent enough across healthcare AI deployments to be predictable - and therefore preventable with deliberate architecture choices made before the first line of code is written.
Model drift. An AI triage model trained on 2024 intake data may start misclassifying complaint types as coding standards, disease prevalence, and patient demographics shift over time. Most teams detect drift 90-180 days after deployment, by which point it has already affected a substantial volume of routing decisions. The fix is automated drift detection with a defined performance threshold that triggers revalidation - not reactive monitoring after accuracy has already visibly degraded.
Edge cases and rare presentations. AI models perform well on high-frequency, high-clarity patterns. Rare chief complaints, atypical presentations, and cases with significant comorbidities that do not fit clean classification categories will be misrouted. Define the confidence threshold below which cases route automatically to human review, and monitor how that threshold performs over time as case mix evolves. Most implementations set this at 75-85% confidence and refine it after the first 60 days of live data.
EHR integration gaps. Most mid-market US clinics run on EHR platforms that were not designed for real-time AI integration. Data extraction relies on HL7 FHIR APIs or file-based exports that are frequently unreliable or delayed at volume. The integration layer - not the model - is where most healthcare AI implementations stall or fail outright. Budget integration and testing work at a minimum of 40% of the total project timeline, and plan for at least one EHR vendor escalation.
Explainability debt. Under GDPR (UK and EU) and emerging CMS guidance in the US, automated decisions affecting clinical pathways must be explainable to patients and reviewers on request. Models that cannot produce a plain-language explanation of their routing decision are a regulatory liability in all three markets. Explainability must be designed into the model architecture from the beginning - retrofitting it after deployment is significantly more expensive and operationally disruptive than building it in.
For a structured pre-deployment review of these risks, the AI workflow automation pre-launch checklist covers the most common failure vectors with concrete remediation steps. Teams evaluating AI automation across the broader healthcare and finance landscape can also reference the AI analytics use cases in healthcare and finance guide for a current view of where the technology is delivering verified ROI versus where it remains experimental.
If your organization is mapping AI workflow automation for patient intake, prior authorization, compliance reporting, or FP&A and financial close processes, our AI automation consulting practice works with health system CIOs, finance directors, and data leads to scope, validate, and deploy automation that is auditable, regulation-compliant, and built to your operational requirements.
---
About Lets Viz: Lets Viz has delivered data analytics and AI automation implementations for US healthcare organizations, UK fintech firms, Canadian manufacturing companies, and global SaaS teams since 2020. The firm holds a 5.0 Clutch rating and specializes in HIPAA-compliant analytics architecture, Microsoft Fabric deployments, and AI workflow automation for mid-market organizations operating across regulated industries.


